
For a substantiated vision with regard to testing, Aviation Covid Collective tries to provide interested parties with more information about the diagnostic methods used. PCR is the foundation of the measures taken with regard to the SARS-CoV-2 virus. The PCR test forms the basis for the statistics on the number of positive tests, infectious persons, R-value, hospital admissions, ICU admissions, deaths and the many models. All forms of testing are calibrated to PCR.
The foundation better be very strong. Basic knowledge and understanding of PCR, and in particular the limitations of PCR, will help to understand that we are cutting corners in many areas. This has enormous social consequences.
The abbreviation PCR stands for ‘polymerase chain reaction’. It is a technique that is used in various laboratories. This technique allows researchers to amplify a tiny amount of DNA until there is enough of it to detect, research, use or analyze. For example, the discovery of PCR has greatly advanced forensic research. In short, PCR is a laboratory technique.
With PCR, specific genetic material (a piece of DNA) can be duplicated by means of a controlled temperature increase and decrease. This doubling step is called a ‘cycle’. The more cycles are performed, the more copies of the piece of DNA are created. Each cycle therefore produces an exponential increase in the amount of genetic material.
To indicate how fast the number of increases is relative to the amount of starting material:
• 1 cycle: twice as much material;
• 2 cycles: 4 x
• 10 cycles: 1024 x
• 20 cycles: 1,048,576 x
• 30 cycles: 1,073,741,824 x
• 40 cycles: 1,099,511,627,776 x
• 45 cycles: 35,184,372,088,832 x
An undetectable amount of DNA can be expanded to a detectable amount by means of PCR. Is there DNA present that you are looking for? Then you will be able to find that with PCR.
Because the SARS-CoV-2 virus is a so-called RNA virus, this RNA has to be converted into DNA by enzymes before it can be multiplied. The enzyme that takes care of this is called ‘reverse transcriptase’ (RT). For this reason, RT-PCR is referred to in the case of amplification of RNA virus material.
A ‘positive’ PCR test is confirmation that a piece of DNA (gene) was present in the sample from the person being tested. It is tested for the ‘presence’ of a gene on the first line of defense of the body, the mucous membranes. Nothing more, nothing less.
The number of cycles required before the specific gene can be detected is called the ‘cycle threshold’ or the Ct value. The Ct value thus provides an indication of the amount of the gene sought in the sample taken. In principle, with a low Ct value (fewer cycles) more of the gene sought was present. If many cycles were required before the gene could be detected, the initial amount was small.
The core of the SARS-CoV-2 coronavirus consists of RNA, made up of many genes. Including N, S, E, RdRP and ORF1a/b genes. [1] The detection of a single piece of gene, e.g. E-gene, does not mean that all other necessary genes required for an intact RNA core are also present. The RNA core of the coronavirus is surrounded by a protein coat. This too is not detected by PCR. PCR therefore never by definition shows intact virus.
A positive test also doesn’t tell you whether the virus has actually entered your cells or whether the viral material is actively multiplying. Without excluding the possibility of other pathogens (such as other viruses) being present, the cause of complaints cannot be attributed to a positive PCR result alone. Also, a positive test does not say whether you are contagious to someone else.
A PCR test result is therefore emphatically not a clinical diagnosis in itself. The manufacturers of PCR test kits are very clear about this in the instructions for use:
“ Positive results are indicative of the presence of SARS-CoV-2 RNA; clinical correlation with patient history and other diagnostic information is necessary to determine patient infection status. Positive results do not rule out bacterial infection or co-infection with other viruses. The agent detected may not be the definite cause of disease.[2]
With regard to public health, the only relevant question should be: when is someone contagious? Contagiousness is a situation with a high virus load and is strongly related to overt complaints, such as a cold or cough. This produces droplets and aerosols that may contain intact viral material.[3]
Cell culture can be used to determine in a lab to what extent someone carries an intact virus and is therefore potentially contagious. [3] Cell culture research is time consuming (1 to 2 weeks) and can only take place in labs with a minimum safety level (BSL-3). For these reasons, not all laboratories are able to carry out this type of research and cell culture on a large scale is therefore impossible.
Various cell culture studies have established a link between Ct value and the extent to which this person may still carry intact virus. [4] [5] [6] A comprehensive study was published in September 2020 linking 3790 positive PCR tests for the E gene and the degree of culturability. [4]
These are the results:
• At Ct value 20: up to 87% can be cultivated;
• At Ct value 25: up to 69% can be cultivated;
• At Ct value 30: up to 22% can be cultivated;
• At Ct value 35: up to 3% can be cultivated;
• With a Ct value higher than 35: no samples can be cultured.
What these results actually show is that of everyone who still tests positive for the E-gene with PCR after 30 cycles, 78% can no longer be contagious. At 35 cycles this increases to 97%. All cell culture studies have one thing in common: the higher the Ct value, the smaller the chance of intact virus.
Interpretation of results
In a publication of March 2021, RIVM states: “Erasmus MC is currently investigating the relationship between the Ct value, the amount of viral RNA and the degree of presence of infectious virus.” [7] It is very strange to say the least that after more than a year and a half of using PCR to diagnose COVID-19, this study has yet to be conducted.[8] Does RIVM see a lack of necessity?
In response to a WOB request, RIVM states that it does not receive the Ct values from laboratories and that it has no knowledge of the distribution of Ct values within the population. [9] However, all positive PCR results are then added together. Until 9 July 2021, a calculation of the number of contagious persons is therefore presented on the Corona Dashboard.[10] Without knowledge of the Ct values, the way in which these figures have been established is indefensible for anyone with basic knowledge of diagnostics (and in particular PCR).
To date, there is still no international standard (SOP) in distinguishing an infectious and non-infectious person. PCR is far from the ‘gold standard’ for making this distinction. [4] [5] [6] [8]
The tests currently used measure the presence of parts of coronavirus on the mucous membranes. When a certain limit value has been reached, the result is called 'positive'.
At present, many travelers (and crews) in commercial aviation are required to undergo pre-testing. These are mostly passengers and crews without corona-related complaints. In the meantime, this concerns millions of tests that have been carried out, with no indication whatsoever between possible infectiousness and a positive result. The policy pursued is in no way consistent with the policy of the RIVM, whereby you are only tested in case of corona-related complaints.
The European Center for Disease Prevention and Control (ECDC), the European equivalent of RIVM, prescribes color coding of countries based on the number of positive tests or ‘cases’.[11] The seriousness of the situation is presented with the colors green, orange, red and dark red. At the end of July 2021, the Netherlands turned dark red. However, a positive test is emphatically not a diagnosis and therefore not a case. A positive test without establishing the relationship with symptoms and a diagnosis made by an expert (doctor) is an empty shell.
On the basis of an enormous amount of test data, of which the RIVM does not seem to know what proportion of this are empty shells, policy is being pursued, the consequences of which are enormous. Not just for aviation, but for society as a whole.
For public health measures, such as quarantine obligations or travel restrictions, it is completely irrelevant whether a person still has a fragment of viral RNA in their nose. To quarantine or impose travel restrictions on someone on the basis of a mere positive PCR test is even morally reprehensible. Several studies show that 50 – 75% of positive PCR tests come from post-infectious individuals.[12][13]
Healthy people without complaints (asymptomatic) are not ill and therefore by definition do not have COVID-19 (Corona Virus Disease). Healthy people without symptoms do not contribute to the spread of the virus.
Of course, someone without symptoms who tests positive can also be in an early stage of an infection and still develop symptoms (presymptomatic). Infectious transmission in asymptomatic individuals is rare and above all, they are never the driving force of a pandemic, according to both WHO and Anthony Fauci. [14][15]
Mass testing of people without symptoms and without further diagnosis from a doctor is a huge mistake from a medical and ethical point of view. The question that must be asked out loud is whether the world has now entered a ’test epidemic’.
On July 26, 2021, The Telegraph in the UK ran a headline: “ Exclusive: Over half of Covid hospitalizations tested positive after admission. ”[16] . As many as 56% of the ‘cases’ were not detected before a standard COVID test was administered to anyone who was admitted for any reason.
Prof Heneghan: “ When people hear about hospitalizations with Covid, they will assume that Covid is the likely cause, but this data shows something quite different – this is about Covid being detected after tests were looking for it. ”
Sir Graham Brady: “ Counting all patients who test positive as Covid hospitalizations is inevitably misleading and gives a false picture of the continuing health impact of the virus. ”
This is no different in the Netherlands:
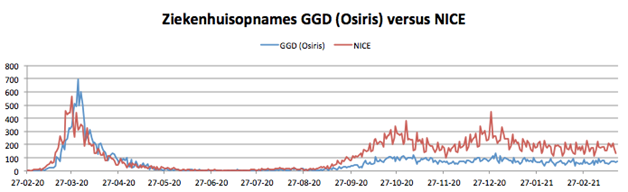
“Until December 16, 2020, the dashboard used figures from the Osiris database. The data in Osiris mainly comes from the GGDs. However, Osiris is significantly underreported of hospital admissions because the GGDs do not always receive more information about hospital admissions of COVID patients.
The NICE file is more complete, but also uses a broader definition of hospitalization. Osiris only includes patients who are hospitalized due to COVID-19, while NICE also reports hospitalizations of patients with COVID-19 who are hospitalized for other reasons. ”[17]
Was there previously significant under-reporting or is there currently over-reporting? It should be clear where this way of counting can lead:[18][19]
We sincerely hope that our concerns about basing policy on test results will find wider support. With large social gaps in knowledge, in our view some restraint and caution in its interpretations is in order.
We ask for understanding for anyone who chooses not to be tested (any longer). Finally, the Aviation Covid Collective requests the interested parties to closely examine their procedures.
Test results are standalone, meaningless.
All forms of testing are calibrated to the PCR method. Test results are standalone, meaningless.
References:
[1] RIVM, Covid-19 Directive, https://lci.rivm.nl/ Guidelines/covid-19
[2] ThermoFisher, TaqPath, COVID‐19 CE‐IVD RT‐PCR Kit, Instructions for use, https://assets.thermofisher.com/TFS-Assets/LSG/manuals/MAN0019215_TaqPathCOVID-19_CE-IVD_RT-PCR%20Kit_IFU. pdf
[3] RIVM, Explanation Sars-CoV-2 PCR, 12 October 2020, https://www.rivm.nl/sites/default/files/2020-11/Toelichting%20PCR_RIVM.pdf
[4] Jaafar et al., Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory Syndrome Coronavirus 2 Isolates, Clinical Infectious Diseases (Volume 72, Issue 11, 1 June 2021, Page e921) , https://doi.org/10.1093/cid/ciaa1491
[5] Bullard et al., Predicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic Samples, Clinical Infectious Diseases (Volume 71, Issue 10, 15 November 2020, Pages 2663–2666), https://doi.org/10.1093/ cid/ciaa638
[6] Singanayagam et al., Duration of infectiousness and correlation with RT-PCR cycle threshold values in cases of COVID-19, England, January to May 2020, Eurosurveillance (13 Aug 2020), https://doi.org/10.2807 /1560-7917.ES.2020.25.32.2001483
[7] RIVM, Status validation SARS-CoV-2 antigen rapid tests, 10 March 2021, https://lci.rivm.nl/sites/default/files/2021-03/Status %20validatie% 20SARS-CoV-2 %20antigeensneltesten% 2010 %20maart% 202021 .pdf
[8] New York Times, Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be., Aug 29, 2020, https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
[9] WOB request to Ministry of Health, Welfare and Sport, by FA Lahr, https://twitter.com/fritsander/status/1407307756588220419?s=20
[10] Central government, Corona Dashboard, Infectious people, https://coronadashboard.rijksoverheid.nl/landelijk/besmetelijke-mensen
[11] European Center for Disease Prevention and Control (ECDC), Maps in support of the Council Recommendation on a coordinated approach to travel measures in the EU, https://www.ecdc.europa.eu/en/covid-19/situation-updates /weekly-maps-coordinated-restriction-free-movement
[12] Stang et al., The performance of the SARS-CoV-2 RT-PCR test as a tool for detecting SARS-CoV-2 infection in the population, Journal of Infection (May 31, 2021), https://doi.org /10.1016/j.jinf.2021.05.022
[13] Mina et al., Clarifying the evidence on SARS-CoV-2 antigen rapid tests in public health responses to COVID-19, The Lancet (Volume 397, Issue 10283, P1425-1427, April 17, 2021), https://doi .org/10.1016/S0140-6736(21)00425-6
[14] WHO, Dr. Maria van Kerkhove, Asymptomatic transmission is very rare, https://www.youtube.com/watch?v=NQTBlbx1Xjs
[15] NIAID, Anthony Fauci, Asymptomatic transmission has NEVER been the driver of outbreaks, https://www.youtube.com/watch?v=vrAvjU2LBkg
[16] The Telegraph, Exclusive: Over half of Covid hospitalizations tested positive after admission, 26 July 2021, https://www.telegraph.co.uk/news/2021/07/26/exclusive-half-covid-hospitalisations-tested-positive -admission/
[17] Central government, Corona Dashboard, Numeracy Hospitals, https://coronadashboard.rijksoverheid.nl/ver Antwoording
[18] NICE Foundation, Hospital admissions, https://stichting-nice.nl/covid-19/public/zkh/new-intake/confirmed
[19] GGD (OSIRIS), Hospital admissions, https://data.rivm.nl/covid-19/COVID-19_aantallen_gemeente_per_dag.csv